
 Clemens M. Schirmer, MD, PhD, FAANS, FAHA (right)
Clemens M. Schirmer, MD, PhD, FAANS, FAHA (right)
Vice-Chair, AANS/CNS Communications and Public Relations Committee
Geisinger Health System
Wilkes Barre, PA
Shelly D. Timmons, MD, PhD, FAANS, FACS (left)
President Elect, AANS
Vice Chair for Administration and Director of Neurotrauma, Department of Neurosurgery at Penn State Milton S. Hershey Medical Center
Hershey, PA
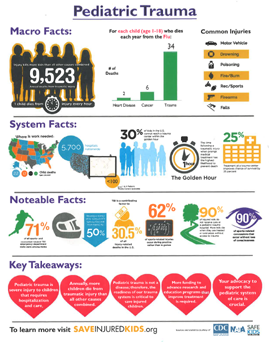
 Pediatric trauma — a severe and potentially life-threatening or disabling injury to a child resulting from an event such as a motor vehicle crash or a fall — is the leading cause of death and disability for children in the U.S. More children die of traumatic injury each year in the U.S. than from all other causes combined, with brain injuries being the most common specific cause of death and disability.
Pediatric trauma — a severe and potentially life-threatening or disabling injury to a child resulting from an event such as a motor vehicle crash or a fall — is the leading cause of death and disability for children in the U.S. More children die of traumatic injury each year in the U.S. than from all other causes combined, with brain injuries being the most common specific cause of death and disability.
Access to timely care is critical in the prevention of death and disability after injury. Only 57 percent of the 73.7 million children in the U.S. during the period 2011-2015 lived within 30 miles of a pediatric trauma center capable of treating all injuries regardless of severity across the spectrum of care; additionally, there is a significant variability between states in this statistic, ranging from above 75 percent to less than 25 percent. In areas without pediatric trauma centers, injured children may have to rely on adult trauma centers or less specialized hospital emergency departments for initial trauma care. Having well-developed trauma systems is therefore critical to provide access to timely neurosurgical and other surgical care, transfer to next-level centers after stabilization and treatment of immediately life-threatening injuries, and provision of specialized services such as rehabilitation after injury.
 It is important to note the difference between an organized trauma system and the identification and maintenance of trauma centers. A trauma system is an integrated system involving multiple components of care, which may be organized on a state, regional, or county level, depending on demography, geography, epidemiology, and governmental or regulatory demands. The mature trauma system includes: pre-hospital management and transport; acute care in hospitals; aftercare in rehabilitation hospitals, physician offices and clinics, and the like; community reintegration programs at home, school, and work; quality improvement mechanisms across this continuum; education and research; and epidemiologically-driven prevention programs based upon regional injury patterns. The maturity of trauma systems and the ways in which they are organized is highly variable across the U.S., and rural areas face particular challenges across the spectrum of care. Caring for injured children is incredibly complex, requires specialized knowledge and equipment, and access to specialty physicians. Because most children die or have permanent disability after trauma from injuries to the brain, involvement of neurosurgeons in not only medical and surgical care, but also in the thoughtful development of systems of care, is crucial.
It is important to note the difference between an organized trauma system and the identification and maintenance of trauma centers. A trauma system is an integrated system involving multiple components of care, which may be organized on a state, regional, or county level, depending on demography, geography, epidemiology, and governmental or regulatory demands. The mature trauma system includes: pre-hospital management and transport; acute care in hospitals; aftercare in rehabilitation hospitals, physician offices and clinics, and the like; community reintegration programs at home, school, and work; quality improvement mechanisms across this continuum; education and research; and epidemiologically-driven prevention programs based upon regional injury patterns. The maturity of trauma systems and the ways in which they are organized is highly variable across the U.S., and rural areas face particular challenges across the spectrum of care. Caring for injured children is incredibly complex, requires specialized knowledge and equipment, and access to specialty physicians. Because most children die or have permanent disability after trauma from injuries to the brain, involvement of neurosurgeons in not only medical and surgical care, but also in the thoughtful development of systems of care, is crucial.
Children are not just “little adults.” Due to several differences that exist between the developing immature brain and the mature adult brain, the impact of injury is different for infants and children. Mechanisms of injury are also different, owing to age-related activities. Therefore, considerations related to acute care and recovery also vary. Examples of differences between pediatric and adult trauma include:
- Mechanisms of Injury: Tend to be lower impact in children from falls, recreational activity, etc., without the complicating factor of intoxication;
- Neurobiology: Differences exist in brain “stiffness” due to myelin maturation water content, neuroreceptor number and distribution;
- Secondary Injury Cascades: Differences may exist in membrane disruption and neurochemical responses, which lead to worsened brain injury in the days and weeks following impact;
- Responses to Treatment: Surgery, medications, and other therapeutics have differing effects on children; and
- Responses to Rehabilitation and Recovery: Children are thought to possess a greater degree of neural plasticity and adaptive capability.
Because of these differences, special attention at all levels of care is essential — particularly in neurotrauma — and systems must address the uniqueness of children and their injuries. Furthermore, since injuries are occurring in a developing brain, and most research is done in mature adults, there is a great deal of research to be done on the impact of various forms of therapeutics in children. These research advancements may also help to establish mechanisms for treatment and restoration of function after common adult brain injuries not only from trauma but other processes such as stroke, Alzheimer’s, Parkinson’s, and others.
There are many challenges to be faced and opportunities for improvement in organization and delivery of pediatric trauma care. These include:
- ensuring adequate and appropriate pre-hospital care for all infants and children;
- providing access to specialty physicians and pediatric trauma centers;
- offering continuing medical education and training for providers at all levels;
- funding research for pediatric traumatic injuries;
- implementing epidemiologically targeted prevention programs;
- evolving appropriate age- and development-related outcomes measures; and
- identifying patient-specific rehabilitation plans and executing them in home environments over the long-term.
As an example of challenges faced in pre-hospital care, one unique challenge is that many emergency medical service vehicles are not fully equipped for pediatric transport. Space for equipment is restricted on both air and ground ambulances, which results in limited availability of all sizes of pediatric airways, cervical spine immobilization devices, and other vital equipment. Furthermore, many emergency responders have limited experience with managing pediatric airways, requiring more frequent education, simulation training, and practice in non-clinical settings. Since airway compromise is a leading cause of preventable death, this is particularly important.
Neurosurgical care is often lifesaving for children suffering from head trauma and brain injuries, and all neurosurgeons are trained to care for injured children, especially in the surgical removal of blood clots that may compress the brain and the prevention and stabilization of brain swelling. Pediatric neurosurgeons have additional training in many aspects of care as relates to infants and children and may assume care from non-specialized neurosurgeons after initial stabilization. Likewise, some neurosurgeons specialize in neurotrauma and neurocritical care and are trained to care for brain injury at all ages. The key is to provide neurosurgical access to all of our population for those time-dependent interventions that save lives, and subsequent sophisticated neurocritical care and neurorehabilitative care to minimize secondary injury and maximize the potential for recovery. This can occur in a variety of configurations and neurosurgeons are actively engaged in designing and implementing trauma systems. However, there is work to be done to provide universal timely and high-quality access to pediatric trauma care through ongoing systems development and support.
 To this end, the AANS and CNS have been founding partners in efforts to establish and promote the efforts of the Congressional Pediatric Trauma Caucus. Representatives from organized neurosurgery, including P. David Adelson, MD, FAANS, and AANS president-elect, Shelly D. Timmons, MD, PhD, FAANS, have participated in several Congressional briefings convened by caucus co-chairs Reps. Richard Hudson (R-N.C.) and G.K. Butterfield (D-N.C.). These events have highlighted the challenges facing pediatric trauma patients and the need to find bipartisan solutions to ensure adequate trauma care for children. As part of this overall effort, the Government Accountability Office (GAO) was tasked with examining various issues related to pediatric trauma. Leaders from the pediatric neurosurgery community provided input to the GAO, including a white paper on pediatric neurotrauma. The resulting GAO report, titled “Availability, Outcomes, and Federal Support Related to Pediatric Trauma Care,” will serve as the basis for future efforts to improve pediatric trauma systems.
To this end, the AANS and CNS have been founding partners in efforts to establish and promote the efforts of the Congressional Pediatric Trauma Caucus. Representatives from organized neurosurgery, including P. David Adelson, MD, FAANS, and AANS president-elect, Shelly D. Timmons, MD, PhD, FAANS, have participated in several Congressional briefings convened by caucus co-chairs Reps. Richard Hudson (R-N.C.) and G.K. Butterfield (D-N.C.). These events have highlighted the challenges facing pediatric trauma patients and the need to find bipartisan solutions to ensure adequate trauma care for children. As part of this overall effort, the Government Accountability Office (GAO) was tasked with examining various issues related to pediatric trauma. Leaders from the pediatric neurosurgery community provided input to the GAO, including a white paper on pediatric neurotrauma. The resulting GAO report, titled “Availability, Outcomes, and Federal Support Related to Pediatric Trauma Care,” will serve as the basis for future efforts to improve pediatric trauma systems.
Our nation’s children deserve the best we have to offer so that they can have every chance of surviving and recovering when they get hurt. America’s neurosurgeons stand at the ready to provide care and to help make vital improvements in our delivery systems.



