
 Uzma Samadani, MD, PhD, FACS, FAANS
Uzma Samadani, MD, PhD, FACS, FAANS
Rockswold Kaplan Endowed Chair, Hennepin County Medical Center
Associate Professor of Neurosurgery, University of Minnesota
Minneapolis, MN
Concussions are a problem. Everyone agrees on that. But it is rather less apparent how to define a concussion accurately, or how to diagnose, track and follow-up post-concussion. Effective treatment is based on the understanding of a clear problem that we are treating and assessing this requires accurate diagnostics, classification schemes, outcome measures and a single definition — all of which have eluded us to this point. Even more daunting is evaluating treatments for a condition that we cannot objectively detect.
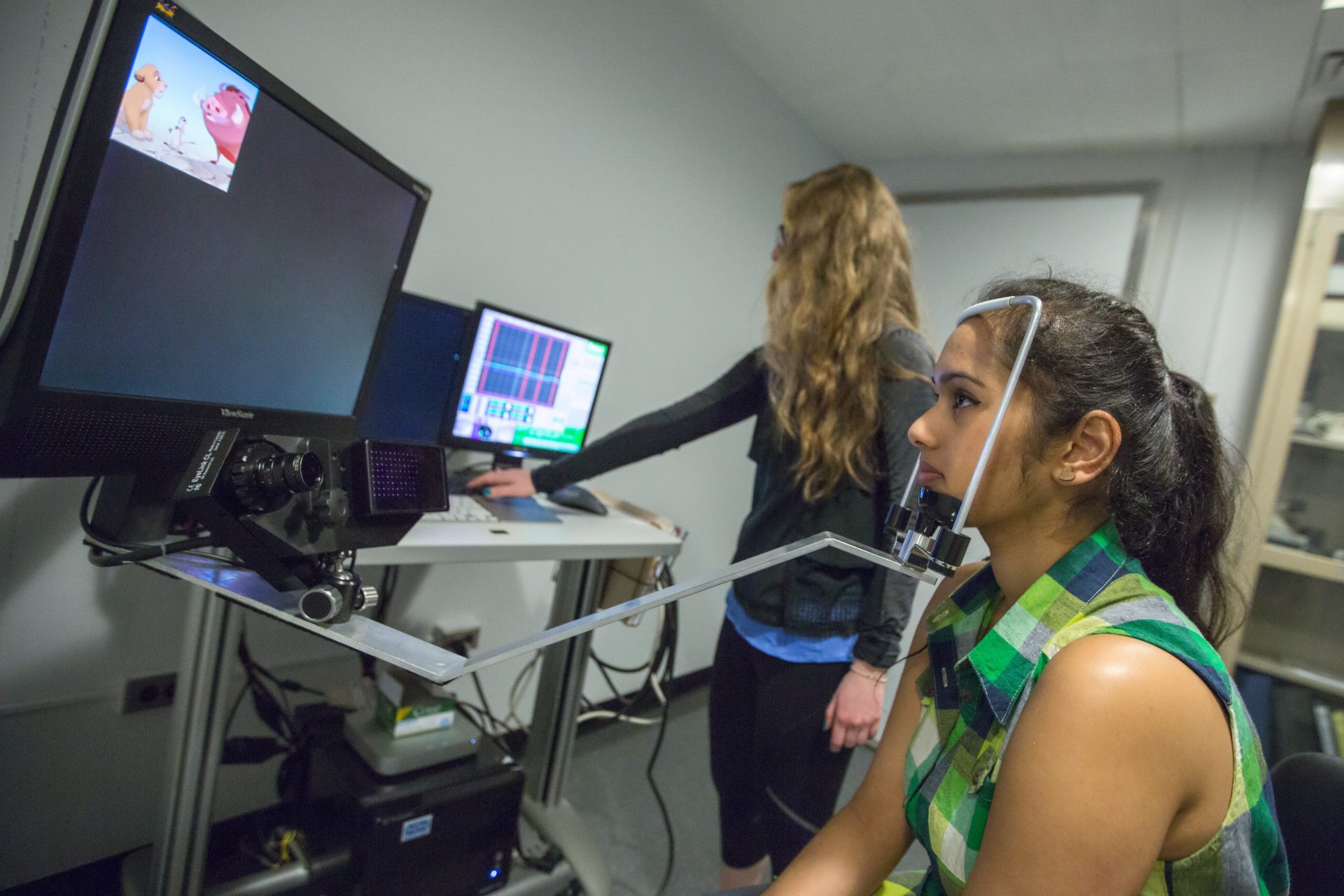
Potential ways for more accurate assessment and classification of traumatic brain injury (TBI) include imaging studies, quantitative EEG, biomarkers, infrared spectroscopy and novel tests. Stepping back, and perhaps away from, using more “big” technology, there has been a renewed interest in eye tracking as a potential diagnostic, biomarker and outcome measure for concussion. To this end, the Hennepin County Medical Center and the University of Minnesota laboratory are contributing to this effort.
The clinical basis for eye tracking as a diagnostic for brain injury has ancient roots. Greek physicians wrote more than 3,500 years ago in the oldest known surviving surgical treatise that eyes that are askew may be indicative of brain injury.1,2 Before the invention of radiographic imaging, the examination of eye movements was a major modality of diagnosis of neurologic impairment with entire textbooks dedicated to this topic.
 Modern era optometrists can detect abnormal eye movements in up to 90 percent of patients with “mild” TBI or concussion.3-8 Following the point in space, such as watching a ping-pong match, requires sustained vergence, or the ability of the both eyes to focus together on a single point. If this point moves closer to the nose, the pupils and eyes will move smoothly together towards the nose or converge. The most commonly detected abnormal eye movement associated with brain injury is a known as a vergence problem.3 Furthermore, studies using eye tracking to assess patients with post-concussive symptoms suggest that these deficits may persist beyond the acute phase of injury.9-11
Modern era optometrists can detect abnormal eye movements in up to 90 percent of patients with “mild” TBI or concussion.3-8 Following the point in space, such as watching a ping-pong match, requires sustained vergence, or the ability of the both eyes to focus together on a single point. If this point moves closer to the nose, the pupils and eyes will move smoothly together towards the nose or converge. The most commonly detected abnormal eye movement associated with brain injury is a known as a vergence problem.3 Furthermore, studies using eye tracking to assess patients with post-concussive symptoms suggest that these deficits may persist beyond the acute phase of injury.9-11
The current generation of eye tracking devices approved by the U.S. Food and Drug Administration (FDA) rely on measurement of visual attention. Our laboratory has recently developed a novel technique that enables detection of palsies (weakness) of the third and sixth cranial nerves whose function it is to contribute to normal eye movements.
Using this technology to evaluate concussions and other head injuries has shown some intriguing and promising results:
- Trauma patients who hit their heads (both positive and negative head CTs) had eye movements that were not as coordinated as uninjured, healthy controls;
- Patients who did not hit their heads had eye movements that were as coordinated as uninjured, healthy controls;
- Statistical analysis demonstrated that the severity of eye movement dysfunction correlated with the severity of concussion symptoms in all trauma subjects; and
- Patients who had hit their heads were found to be worse in the 1-2 weeks following injury and then gradually recovered towards normal within the next month.13
Results further demonstrated that more than two-thirds of the patients who are evaluated in an emergency department for mild TBI requiring brain imaging have normal eye tracking, suggesting physiologically normal brain function. As many of these patients still complain of headache, nausea, vomiting or dizziness, this research suggests these symptoms may have multifactorial causes, for example, from scalp, neck, inner ear, pain or visceral causes.
 The current thinking in medicine is that objective measures and data will drive diagnostics in health care, as they are less subject to human interpretation and bias and offer a reproducible metric to assess how well we are doing with treatment going forward. Objective measures of radiographically silent neurologic disruption will enable more precise definition of concussion, something much needed as currently there are more than 42 organizations that have developed definitions of concussion without coming to a consensus. Many of these definitions encompass any symptoms related to scalp, neck, inner ear, or other systemic problems, as well as brain injury. Thus, eye tracking might ultimately be used to help classify or even define concussion, in conjunction with other modalities.
The current thinking in medicine is that objective measures and data will drive diagnostics in health care, as they are less subject to human interpretation and bias and offer a reproducible metric to assess how well we are doing with treatment going forward. Objective measures of radiographically silent neurologic disruption will enable more precise definition of concussion, something much needed as currently there are more than 42 organizations that have developed definitions of concussion without coming to a consensus. Many of these definitions encompass any symptoms related to scalp, neck, inner ear, or other systemic problems, as well as brain injury. Thus, eye tracking might ultimately be used to help classify or even define concussion, in conjunction with other modalities.
A critical implication of any test that distinguishes patients with concussion caused by actual brain injury is improved quantitative evaluation of clinical trials and outcomes. Similarly, improved classification of patients with structural brain injury enrolling in trials is also enabled with eye tracking. Many innovative and dedicated neurosurgeons are committed to the care of head injured patients and have taken on this challenge, with considerable promise. Neurosurgeons continue to lead the way in both clinical care of patients with concussions and with critical research to enable improved evaluation and outcomes.
Editor’s Note: We encourage everyone to join the conversation online by using the hashtag #ConcussionFacts.
References:
- Kamp MA, Tahsim-Oglou Y, Steiger HJ, Hanggi D. Traumatic brain injuries in the ancient Egypt: insights from the Edwin Smith Papyrus. Journal of neurological surgery. Part A, Central European neurosurgery. 2012;73(4):230-237.
- Sanchez GM, Burridge AL. Decision making in head injury management in the Edwin Smith Papyrus. Neurosurgical focus. 2007;23(1):E5.
- Thiagarajan P, Ciuffreda KJ, Ludlam DP. Vergence dysfunction in mild traumatic brain injury (mTBI): a review. Ophthalmic Physiol Opt. 2011;31(5):456-468.
- Ciuffreda KJ, Rutner D, Kapoor N, Suchoff IB, Craig S, Han ME. Vision therapy for oculomotor dysfunctions in acquired brain injury: a retrospective analysis. Optometry. 2008;79(1):18-22.
- Goodrich GL, Flyg HM, Kirby JE, Chang CY, Martinsen GL. Mechanisms of TBI and visual consequences in military and veteran populations. Optometry and vision science : official publication of the American Academy of Optometry. 2013;90(2):105-112.
- Alvarez TL, Kim EH, Vicci VR, Dhar SK, Biswal BB, Barrett AM. Concurrent vision dysfunctions in convergence insufficiency with traumatic brain injury. Optometry and vision science : official publication of the American Academy of Optometry. 2012;89(12):1740-1751.
- Suh M, Basu S, Kolster R, Sarkar R, McCandliss B, Ghajar J. Increased oculomotor deficits during target blanking as an indicator of mild traumatic brain injury. Neuroscience letters. 2006;410(3):203-207.
- Suh M, Kolster R, Sarkar R, McCandliss B, Ghajar J. Deficits in predictive smooth pursuit after mild traumatic brain injury. Neuroscience letters. 2006;401(1-2):108-113.
- Heitger MH, Jones RD, Macleod AD, Snell DL, Frampton CM, Anderson TJ. Impaired eye movements in post-concussion syndrome indicate suboptimal brain function beyond the influence of depression, malingering or intellectual ability. Brain : a journal of neurology. 2009;132(Pt 10):2850-2870.
- Cifu DX, Wares JR, Hoke KW, Wetzel PA, Gitchel G, Carne W. Differential eye movements in mild traumatic brain injury versus normal controls. The Journal of head trauma rehabilitation. 2015;30(1):21-28.
- Cifu DX, Hoke KW, Wetzel PA, Wares JR, Gitchel G, Carne W. Effects of hyperbaric oxygen on eye tracking abnormalities in males after mild traumatic brain injury. J Rehabil Res Dev. 2014;



